A practical approach to Respiratory Function Testing
Introduction
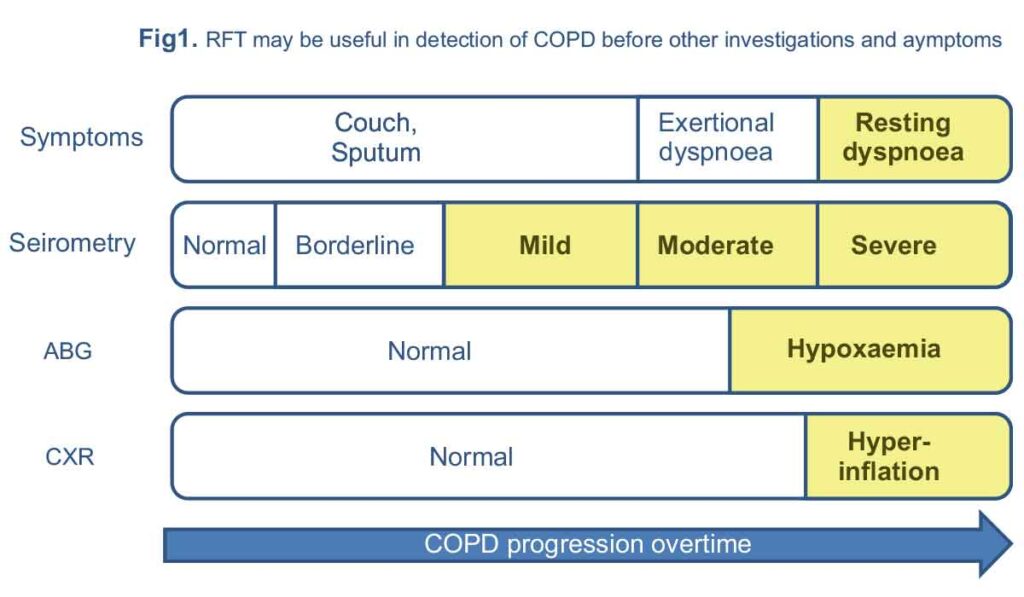
Although respiratory function tests are an integral part of diagnosis and management of respiratory diseases, they are not diagnostic for any given disease. Respiratory function tests may be able to identify and quantify respiratory system functional abnormalities years before other investigations become abnormal or patients become worry about their symptoms (figure 1).
Respiratory Function Test
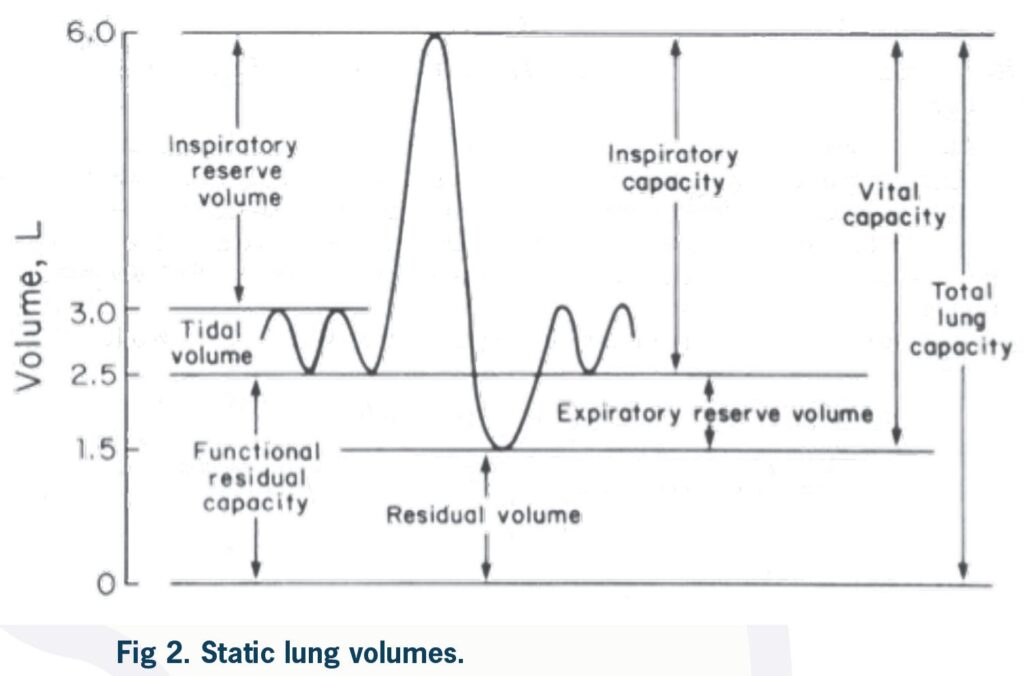
Lung Volumes and capacities
Spirometry
Testing
Spirometry is a tool to assess ventilatory function by measurement of inspired and expired volumes over time (i.e. dynamic lung volumes). A subject is asked to inspire maximally and then exhale forcefully and completely into a spirometer.
Volume measurements
Flow measurements
Baseline values
The baseline values for each patient are determined by patient age, sex, height and ethnicity.
After entering these parameters to the device, the baseline (normal) predicted values for a particular patient are calculated and the results of patient’s test are compared with these normal values and presented as percentages and also raw numbers.
The baseline values have been well validated in population studies for Caucasians. In non-Caucasian population a correction factor is used. These baseline values are validated for patients between 8Ð80 years of age and values beyond these age groups are extrapolated.
This may cause some degree of inaccuracy in interpretation of lung function tests in these age groups.
Test performance
Interpretation
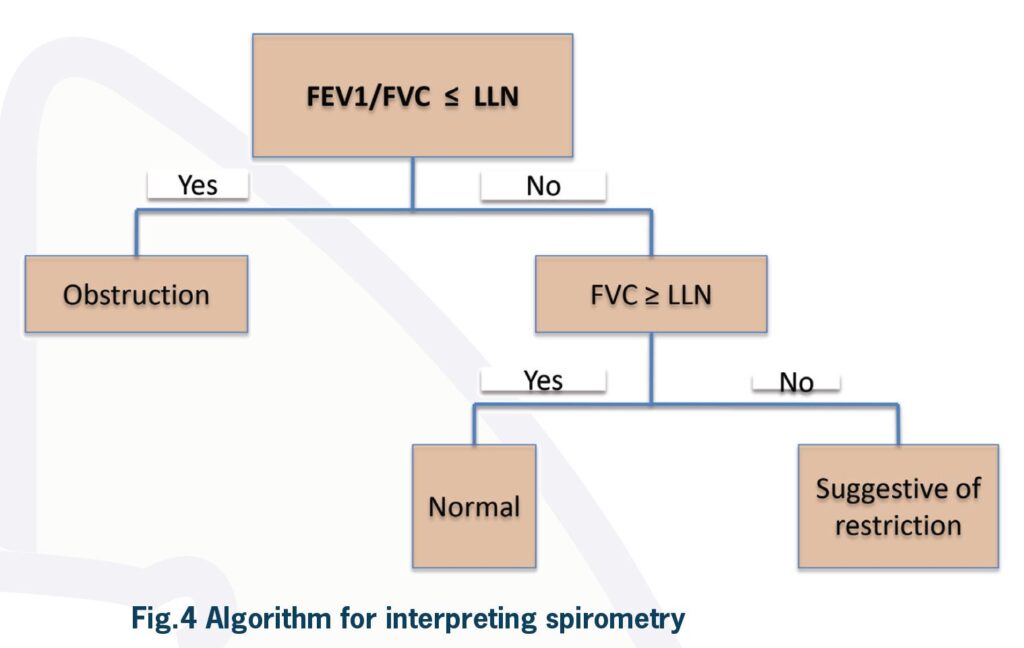
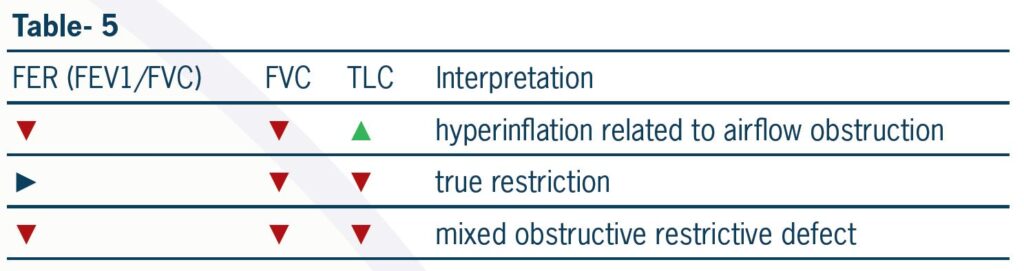
If FER is not reduced to less than what is predicted for the patient, then an obstructive ventilatory defect is ruled out. This result can be seen in a normal patient or patients with restrictive defects. Looking at vital capacity (VC) or FVC is the next step to differentiate between these two. If FVC or VC is less than lower limit of normal for a particular patient and FER is normal, spirometry is suggestive of restrictive ventilatory defect. This finding has to be confirmed by measurement of total lung capacity which is the gold standard for diagnosis of restriction. Normal VC or FVC rules out restrictive defect.
Reduced FVC when FER is reduced most likely indicate hyperinflation as a result of severe airflow obstruction. It may also be due to a mixed ventilatory defect. Measurement of lung volumes is necessary to differentiate between these. A mixed obstructive and restrictive ventilatory defect is present when both FER and TLC are reduced.
There are patients who do not follow the above algorithm. Normal spirometry does not exclude severe lung disease. For example in a subgroup of patients with combined Emphysema and Interstitial Lung Disease there is a relative preservation of lung volumes with normal spirometry and marked reduction in DLCO . However, these group of patients will have severe limitation in gas transfer properties, which will be discussed later in this article.
After one is diagnosed with airflow obstruction (FER<lower limit of normal), the next step is to classify the severity of obstructive defect and to assess for presence of bronchodilator response (suggestive of current asthma).
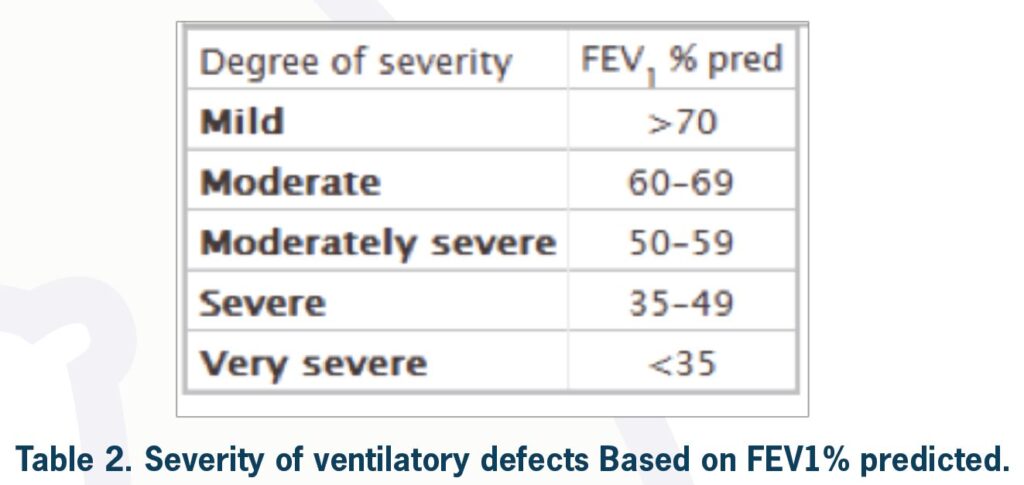
Severity of limitation
To classify the severity of a ventilatory defect one needs to look at FEV1% predicted for the patient. According to ATS/ERS task force, the degree of severity is as shown in table 2.
As an example if a patient has FER<predicted LLN and FEV1=100% predicted, by definition this patient has mild obstructive ventilatory defect (although this can be considered a normal variant depending clinical information). However, this can be sometimes considered normal especially in young population.
Bronchodilator response
Spirometry can be performed before and after the administration of an inhaled bronchodilator to test for a significant response, which is suggestive of reversible airflow obstruction. To assess bronchodilator response the patient is given 400 microgram of inhaled salbutamol (four separate puffs with 30 seconds intervals) via spacer and spirometry is repeated after 15 minutes. If FEV1 and/or FVC is improved by more than 200 millilitres and 12% after salbutamol use, bronchodilator response is positive. This is suggestive of bronchial hyper-reactivity. In an appropriate setting this result can be consistent with un-controlled asthma. Bronchial hyper-responsiveness has clinical implications. It may suggest benefit from further treatment with inhaled corticosteroids or addition of long acting bronchodilators.
If the clinician is looking for reversibility in lung function to investigate their patient for possible asthma, the patients should not take their short acting bronchodilator 4-6 hours before spirometry and long acting bronchodilator 12-24 hours prior to testing.
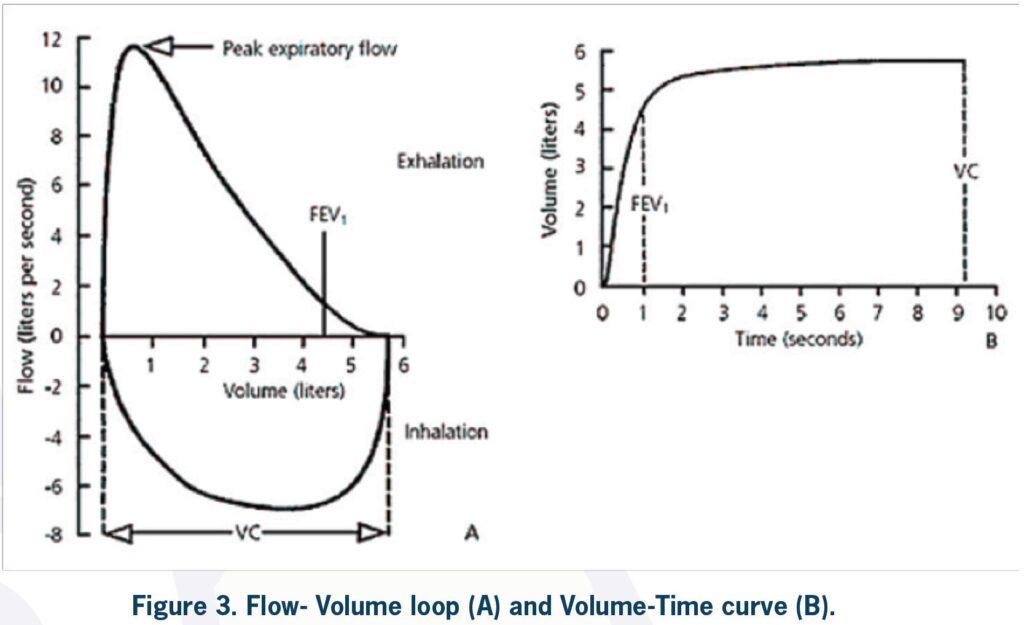
Review of flow volume loop (FVL)
Pathologic FVLs
Diffusing capacity
Carbon monoxide is the gas used to measure diffusing capacity of the lung (“window on the pulmonary microcirculation”).
Because of its high affinity to haemoglobin, carbon monoxide is considered a diffusion-limited gas. Nitrogen and oxygen are considered perfusion limited and both perfusion/diffusion limited gases retrospectively.
Carbon monoxide has 200 times more binding affinity to haemoglobin compared to oxygen. This property of carbon monoxide prevents high concentration of the gas in the capillary blood and tension across membranes does not occur.
So gas concentration is not usually a limiting factor for its transfer across alveolar capillary membrane. The causes of limitation in diffusing capacity for carbon monoxide (DLCO ) are listed in table 3.
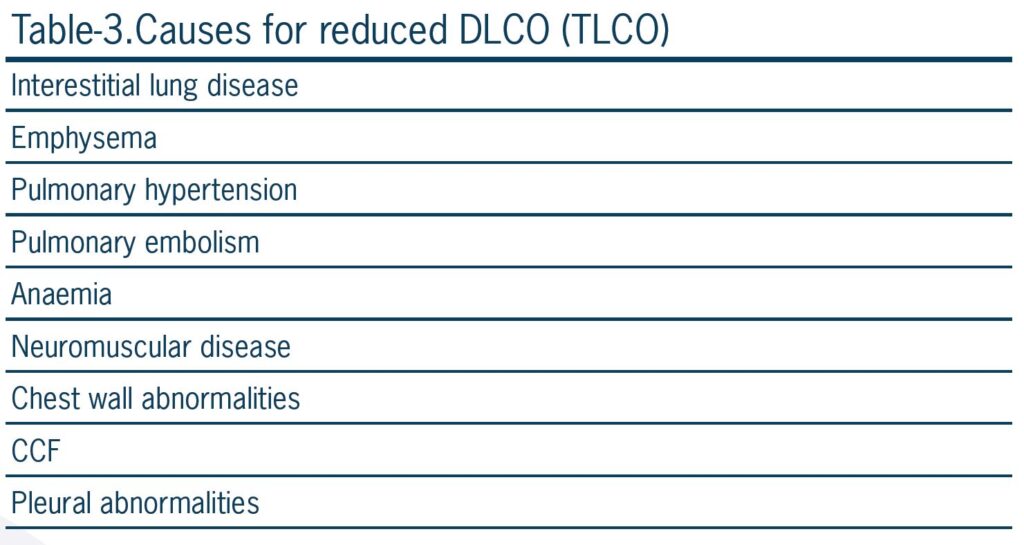
(TLCO = Transfer factor for carbon monoxide) Similar to normal values for spirometry, DLCO predicted values determined by patient’s sex, age, height, ethnicity and altitude (inspired oxygen concentration). There are many other factors that can affect DLCO including circadian rhythm, menstrual cycle, smoking, bronchodilator use, exercise, haemoglobin concentration, carboxyhaemoglobin concentration, body position and obesity in women (due to overestimation of the normal value for DLCO in obese women).
In many respiratory laboratories haemoglobin concentration is measured by a finger prick test and measure DLCO is corrected for haemoglobin. Clinicians always look for corrected DLCO to assess diffusion limitation.
It is also important to correct DLCO for alveolar (lung) volume (VA). In most cases with reduced lung volume DLCO is also reduced.
It is not clear whether the reduction in diffusion capacity is due to extrathoracic causes (including chest wall and pleural abnormality, neuromuscular disease or poor test performance) or real reduction in diffusion capacity.
If DLCO corrected for alveolar volume (KCO= DLCO/VA) is also reduced it is suggestive of paranchymal or pulmonary vascular disease.

Lung volumes
Bronchial Challenge Tests
There are two types of bronchial challenge tests. Indirect challenges which activate mast cells to release histamine and other bronchoconstrictor mediators (e.g. mannitol, hypertonic saline, eucapnic voluntary hyperventilation, exercise challenge).
Direct challenges, which directly constrict airway smooth muscle via receptors on smooth muscle (e.g. methacholine, histamine).
These tests are considered positive if a known dose of stimuli can cause a 20% (direct challenge) or 15% (indirect challenge) reduction in FEV1. These test are useful in excluding, rather than confirming, a diagnosis of asthma.
There are 2 components of airway hyper-responsiveness, inflammation and persistent airway remodelling. A greater change in responsiveness to indirect stimuli (e.g. mannitol, hypertonic saline) is suggestive of more inflammatory component and need for treatment with inhaled corticosteroids.
On the other hand greater response to direct airway stimuli (methacholine, histamine) is suggestive of persistent airway remodelling. Response to direct stimuli may decreases during treatment with ICS but it does not resolve.
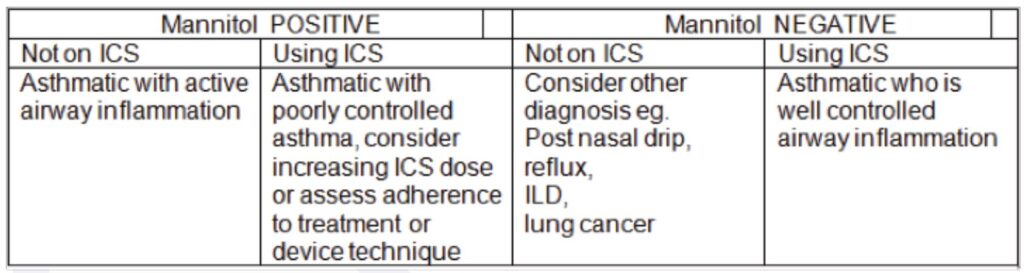
A positive indirect test is consistent with a diagnosis of active asthma (high specificity) and predicts respond to treatment with inhaled steroids. They are also used in diagnosing exercise-induced bronchoconstriction (EIB) and identifying individuals who may experience “airway narrowing” while SCUBA diving.
Table-6 shows some clinical advantages of mannitol challenge test in diagnosis and management of patients with respiratory disorders.
In an asthmatic patient with a normal lung function and negative indirect challenge test a regular long-acting b 2 –agonist is probably not warranted.
Patients follow up and repeat RFTs to assess progression of disease.
One of the main indications for respiratory function tests is in following up the patients and screening for progression of chronic lung diseases.
In obstructive lung disease a decline in FEV1 by more than 12% and 200ml is considered significant. As a general rule a decline in DLCO by more than 3 units is considered significant.
A positive bronchodilator response or a positive bronchial challenge test in an asthmatic suggest current airway hyper-responsiveness and need for further therapy.
In idiopathic pulmonary fibrosis, FVC and TLC correlate poorly with morphologic extent of disease on HRCT and are less predictive of outcome than DLCO. A 10% change in FVC or 15% change in TLCO is considered significant in management of interstitial lung disease.
DLCO is a good parameter in following up of patients with combined emphysema and interstitial lung disease and ILD combined with pulmonary hypertension.
About Us
At RSDC we have a particular interest in quick approach and triaging patients with suspected lung malignancy, management of pleural diseases, sleep disorders of obstructive sleep apnoea and other more complex sleep disorders, airways disease including asthma and COPD.
We use a comprehensive approach to interstitial lung disease in addition to occupational and environmental lung disease.
