
Cardiopulmonary Exercise Testing (CPET)

CPET involves measurements of the cardiac, metabolic, and respiratory systems while the patient exercises to maximum capacity. CPET may be a useful tool for the following:
Assessing the risk to patients having surgery (perioperative assessment)
Determining causes for unexplained dyspnoea
Assessing the contribution of cardiac or respiratory causes to incapacity
Quantifying the extent of impairment
Measuring the response to and efficacy of an intervention
A comprehensive report and conclusion will be provided to the referring practitioner.
Please note: Patients with known cardiac disease, who are at risk of cardiac events when exercising at maximum capacity, may not be able to undertake this test.
Spirometry
Spirometry measures the flow and volume of air entering and leaving the lungs. It is used to assess the ventilatory function of a patient and to differentiate between possible obstructive or restrictive defects.
Indications for Spirometry:
Evaluation of symptoms such as dyspnea, cough, wheeze, and sputum production
To assess known disease progression
To monitor the efficacy of interventions
Airway reversibility is tested using Ventolin Stepwise approach to interpreting Spirometry
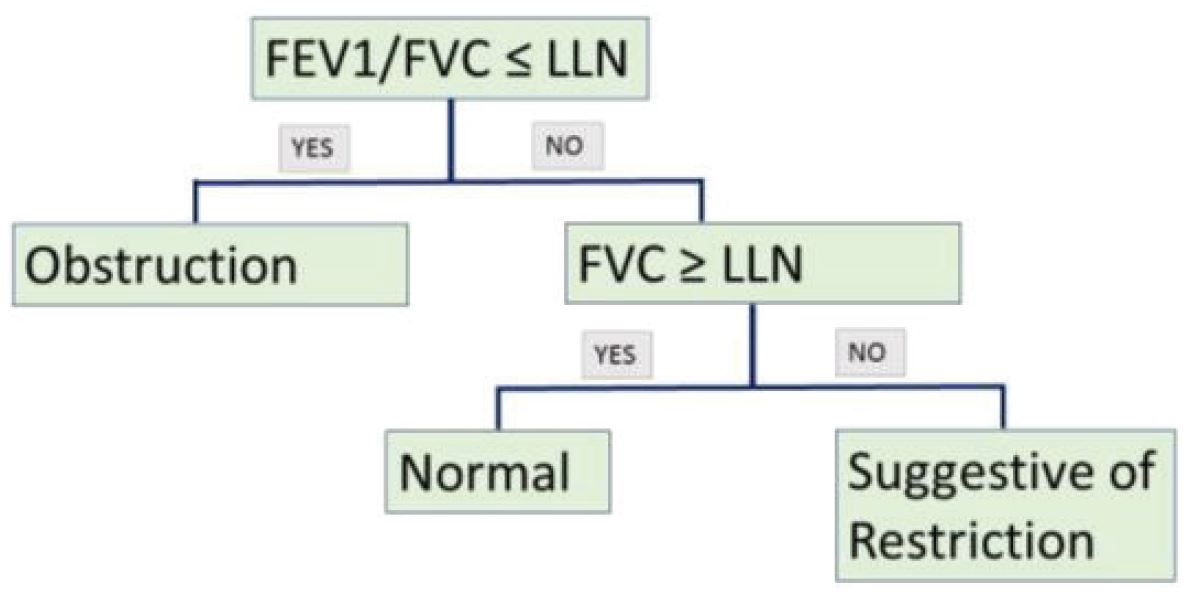
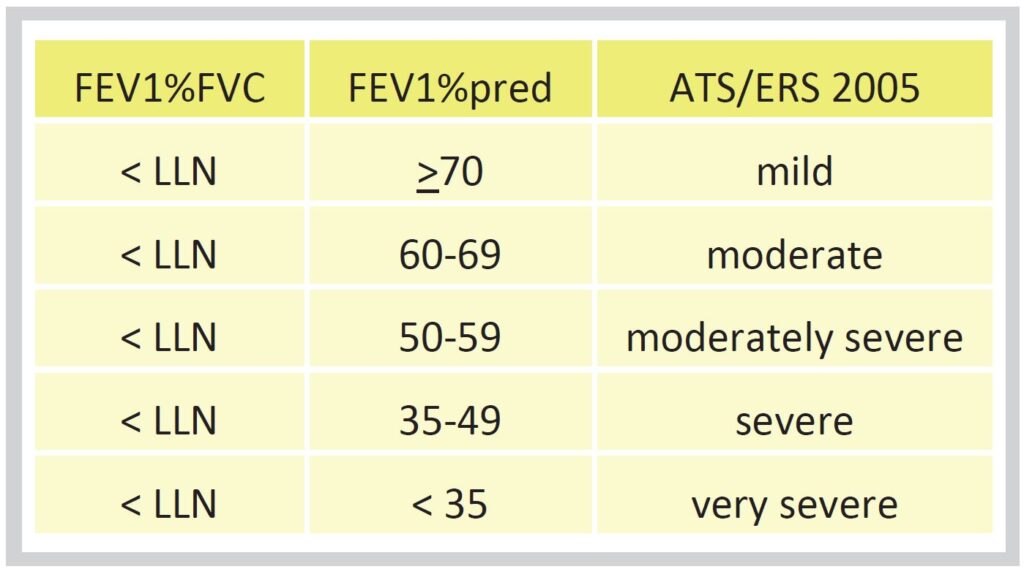
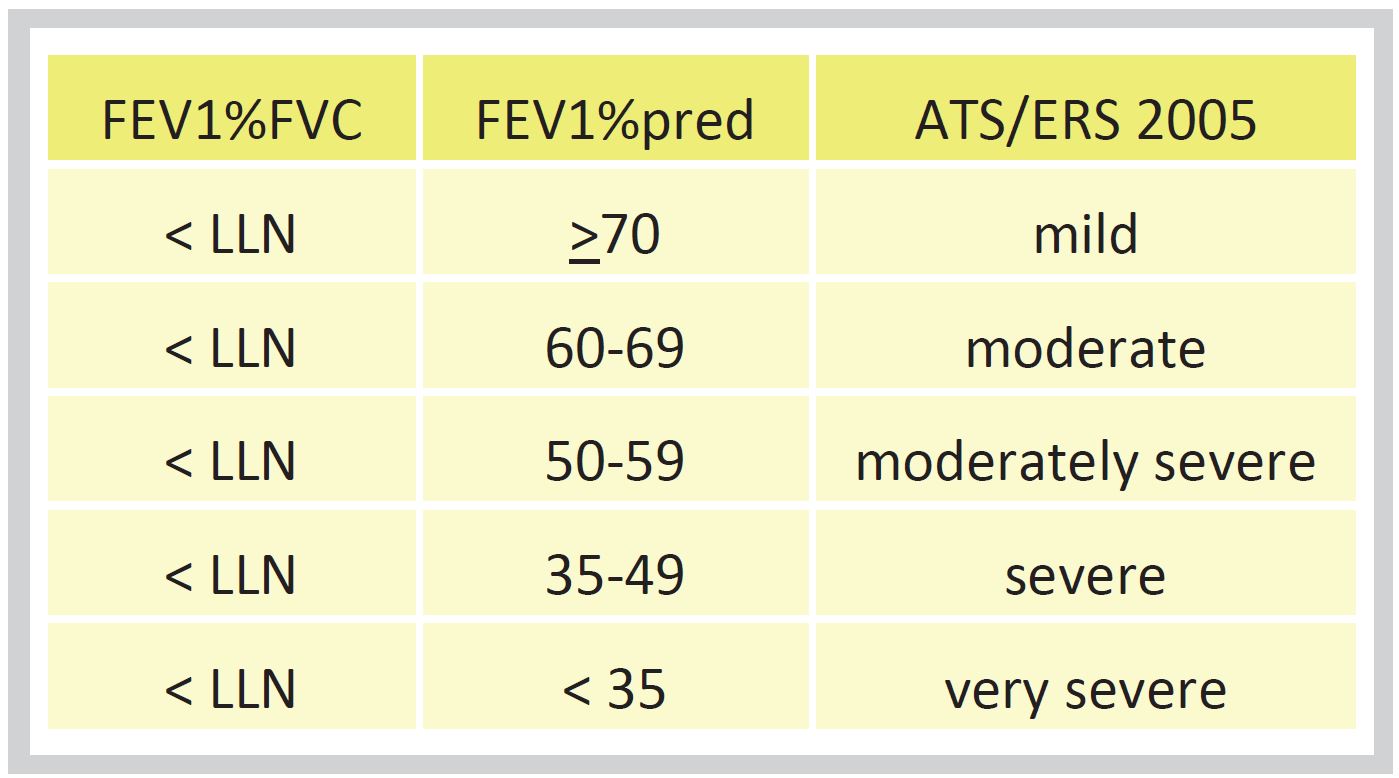
Severity of Obstruction
Gas Transfer
Diffusing capacity for carbon monoxide (DLCO) measures the ability of the lung to transport oxygen from the alveoli into the bloodstream. DLCO can be reduced due to many causes, including:
Interstitial lung disease
Emphysema
Pulmonary hypertension
Pulmonary embolism
Congestive cardiac failure
Anaemia
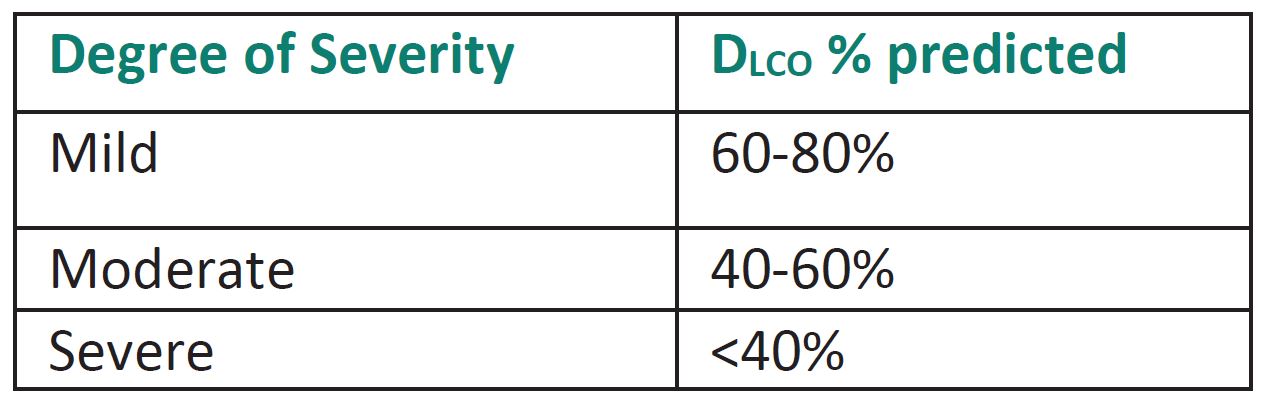
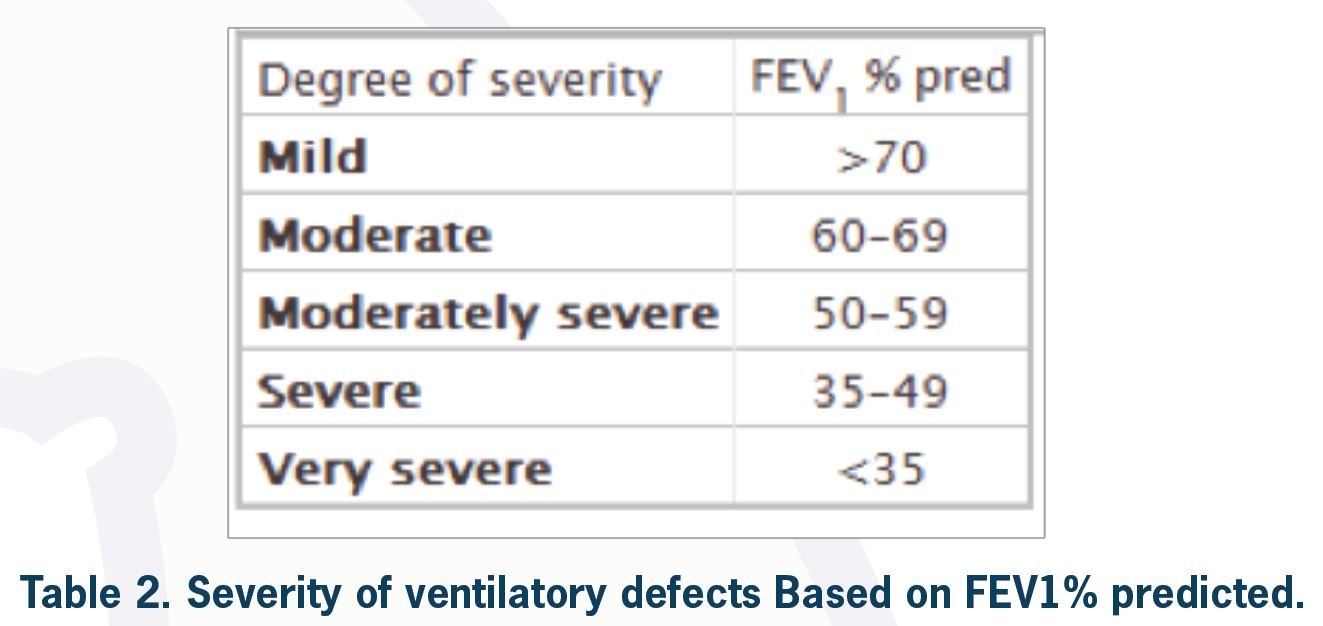
Severity of Limitation
To classify the severity of a ventilatory defect, one needs to look at FEV1% predicted for the patient. According to the ATS/ERS task force, the degree of severity is as shown in Table 2.
Example: If a patient has FER < predicted LLN and FEV1 = 100% predicted, by definition, this patient has a mild obstructive ventilatory defect (although this can be considered a normal variant depending on clinical information). However, this can sometimes be considered normal, especially in young populations.
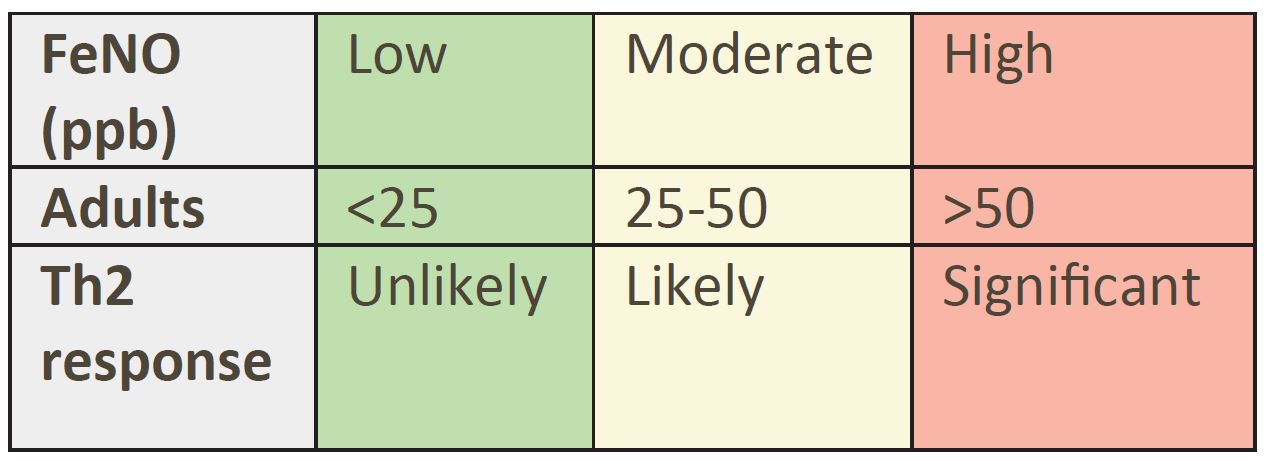
Expired Nitric Oxide (FeNO)
Expired Nitric Oxide (FeNO) is considered an important biomarker of airway eosinophilic inflammation.
Measurement of FeNO assists in phenotyping asthma and determining corticosteroid responsiveness.
FeNO may also indicate exposure to allergens.
Flow Volume Loops (FVL)
As mentioned previously, useful information regarding test performance and artefacts during spirometry can be obtained by looking at FVL. Flow volume loops are also valuable in diagnosing upper airway (intrathoracic or extrathoracic) pathologies.
Lung Volumes
Measurement of absolute lung volumes is obtained using body plethysmography.
This test is required to confirm or rule out true restriction.
Lung volumes are important to quantify gas trapping.

MIPS and MEPS
Maximum Inspiratory Pressure (MIP) and Maximum Expiratory Pressure (MEP) measurements are used to assess muscle strength within the respiratory system and diagnose diseases of these muscles.
It is useful in the following conditions:
Respiratory muscle weakness or neuromuscular disease is suspected.
Lung function tests show reduced vital capacity with normal gas transfer.
Assess if known respiratory muscle weakness has improved, remained stable, or worsened.
